Last updated on Jul 20, 2026
FL DFS-F2-DWC-1 2009-2026 free printable template
pdfFiller is not affiliated with any government organization
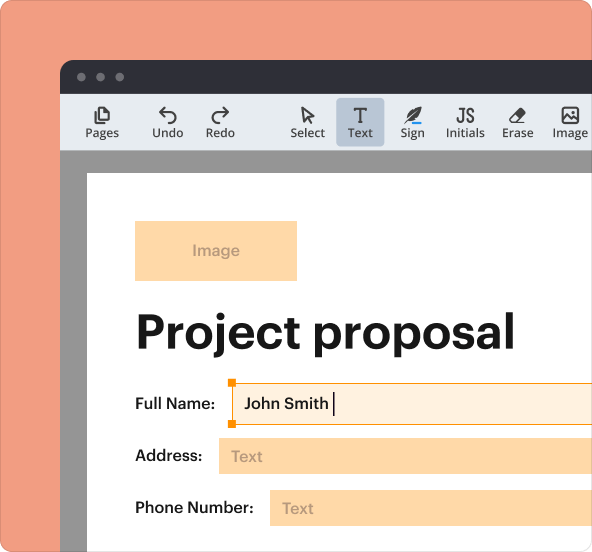
Fill out
Complete the form online in a simple drag-and-drop editor.
eSign
Add your legally binding signature or send the form for signing.
Share
Share the form via a link, letting anyone fill it out from any device.
Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
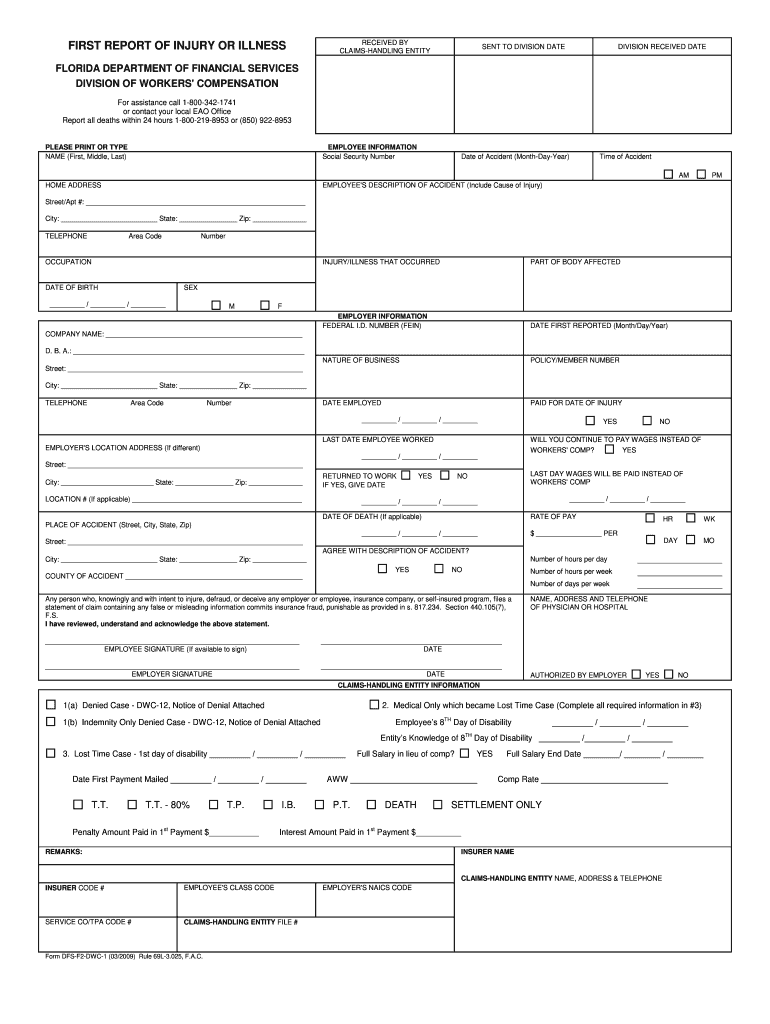
What is FL DFS-F2-DWC-1
The Florida First Report of Injury or Illness is a healthcare form used by employees and employers to report work-related injuries or illnesses to the Florida Division of Workers' Compensation.
pdfFiller scores top ratings on review platforms
Who needs FL DFS-F2-DWC-1?
Explore how professionals across industries use pdfFiller.

FL DFS-F2-DWC-1 is needed by:
-
Employees filing for work injury reports in Florida
-
Employers managing workplace injury claims
-
Workers' compensation insurance providers
-
HR departments in Florida-based companies
-
Legal professionals advising on workers' compensation
Comprehensive Guide to FL DFS-F2-DWC-1
What is the Florida First Report of Injury or Illness?
The Florida First Report of Injury or Illness, officially known as Form DFS-F2-DWC-1, is a critical document in the Florida workers' compensation process. This form serves to report work-related injuries or illnesses, ensuring that employees receive the necessary medical care and benefits. Timely submission of this form is essential for both employees and employers as it triggers the worker's compensation claim process, allowing for appropriate benefits to be administered.
Purpose and Benefits of the Florida First Report of Injury or Illness
Accurate reporting using the Florida First Report facilitates effective communication between the employee, employer, and insurance providers. When filed correctly, it not only helps in documenting the incident but also has significant legal implications. Ensuring all parties fulfill their obligations can prevent disputes and foster a smoother compensation process.
Who Needs to Complete the Florida First Report of Injury or Illness?
Both employees and employers have defined roles in completing the Florida First Report. Each party is required to fill out and sign the form, highlighting their responsibilities in the reporting process. This collaboration assures that the necessary information is accurately captured to support the claim.
How to Fill Out the Florida First Report of Injury or Illness Online (Step-by-Step)
To fill out the Florida First Report online, you can use platforms like pdfFiller. Follow these steps:
-
Access the form using a web browser.
-
Enter the necessary employee details such as name and contact information.
-
Complete sections detailing the accident, including date, time, and nature of the injury.
-
Provide the employer's details, ensuring accurate representation.
-
Sign the form using eSignature capabilities offered by the platform.
-
Review and submit the completed form.
Field-by-Field Instructions for Completing the Florida First Report of Injury or Illness
Understanding the specific fields on the Florida First Report is crucial for accurate completion. Key fields include:
-
NAME: Gather the employee's full name (First, Middle, Last).
-
EMPLOYEE SIGNATURE: Ensure the employee signs on the designated line.
-
EMPLOYER SIGNATURE: The employer must also provide a signature to validate the report.
Avoid common errors such as leaving required fields blank or providing incorrect information, which can delay processing.
Submission Methods for the Florida First Report of Injury or Illness
Once the Florida First Report is completed, there are several methods for submission:
-
Online submission through approved platforms.
-
Mailing a hard copy to the relevant office.
-
Faxing the completed form to the state’s workers' compensation division.
Be aware of important deadlines to ensure compliance with state regulations.
Consequences of Not Filing or Late Filing the Florida First Report of Injury or Illness
Failure to file the Florida First Report on time can lead to serious repercussions for both employees and employers. Potential consequences include:
-
Legal actions taken against the employer.
-
Loss of benefits or compensation for the injured employee.
-
Increased scrutiny from regulatory agencies.
Maintaining accurate records and complying with filing deadlines is imperative to avoid these issues.
How pdfFiller Simplifies the Completion of the Florida First Report of Injury or Illness
pdfFiller offers a range of features that make filling out the Florida First Report straightforward. Key benefits include:
-
User-friendly interface for easy form navigation.
-
eSigning functionalities for quick and secure sign-off.
-
Document management to keep all forms organized.
The platform ensures compliance and security through 256-bit encryption and adherence to regulations like HIPAA and GDPR.
Final Steps and What to Expect After Submitting the Florida First Report of Injury or Illness
After submitting the Florida First Report, it's important to follow up. You should:
-
Track the submission status via the platform used.
-
Anticipate the timeline for responses from the insurance provider.
-
Prepare for potential follow-up actions if the form is rejected.
Staying proactive can help ensure any issues are addressed promptly.
Sample Completed Florida First Report of Injury or Illness for Reference
Providing a visual aid, a sample completed Florida First Report can be immensely helpful. This example includes:
-
A filled-out form with hypothetical data for clarity.
-
Annotations that explain the significance of various sections and fields.
Referencing a sample can assist users in understanding the expectations for their own submissions.
How to fill out the FL DFS-F2-DWC-1
-
1.Access pdfFiller and log in to your account. If you are new, create an account for free.
-
2.Search for 'Florida First Report of Injury or Illness' or use the form ID 'DFS-F2-DWC-1' in the search bar.
-
3.Once the form loads, review the form layout to familiarize yourself with the sections.
-
4.Gather all necessary information, including details of the injured employee, the nature of the injury, and employer information.
-
5.Begin filling in the employee's information, including their full name, job title, and contact details in the designated fields.
-
6.Next, provide a detailed description of the injury or illness, including the date, time, and circumstances of the event.
-
7.Proceed to provide the employer's information, ensuring accurate company details and contact information is included.
-
8.Utilize the checkboxes to indicate any potential witnesses or prior related injuries if required.
-
9.Review each field for any errors or incomplete sections to ensure accuracy before finalizing the document.
-
10.Once everything is complete, both the employee and employer should sign the form using pdfFiller’s built-in e-signature tool.
-
11.After signing, review the document one final time, making any necessary adjustments.
-
12.Save the completed form as a PDF, and use pdfFiller’s options to download or print a copy for your records.
-
13.Lastly, submit the form according to your employer’s guidelines or send it directly to the Florida Division of Workers' Compensation as required.
Who is required to complete the Florida First Report of Injury or Illness?
Both the employee and employer are required to complete and sign the Florida First Report of Injury or Illness. This ensures that both parties acknowledge the details of the injury or illness being reported.
What information do I need to complete this form?
You need the employee's name, contact information, job title, details of the injury or illness, time, and circumstances surrounding the incident, as well as the employer’s details. Ensure you have all relevant information ready before starting.
What are the submission methods for this form?
The completed Florida First Report of Injury or Illness can be submitted directly to the Florida Division of Workers' Compensation. It can also be provided to the employer’s HR department, depending on company policies.
Are there deadlines for submitting this form?
Yes, the form should be submitted as soon as the injury or illness is known to ensure compliance with state regulations. Delays in reporting may affect claim eligibility for workers' compensation benefits.
What are common mistakes to avoid when filling out this form?
Common mistakes include leaving fields blank, providing incorrect or incomplete information, and not ensuring both the employee and employer signatures are present. Always double-check for accuracy before submission.
How long does it take for the report to be processed?
Processing times can vary, but the Florida Division of Workers' Compensation generally reviews reports within a few business days. Keep copies of your submission for follow-up purposes.
Is notarization required for this form?
No, the Florida First Report of Injury or Illness does not require notarization. It only needs signatures from both the employee and the employer.
Related Content
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.